
For general education, not medical advice. This guide can’t diagnose you or replace care from your own clinician. If you’re worried about a spot or symptom, see a board-certified dermatologist.
Basal cell carcinoma (BCC) is the most common skin cancer. It starts in the basal cells at the base of the outer skin layer, usually on sun-exposed areas like the face, ears, neck, and hands. It grows slowly and rarely spreads to other parts of the body. But left alone, it can grow into nearby skin, cartilage, and bone. The good news: caught early, it is highly curable.
Key points
- BCC is the most common skin cancer; it grows slowly and rarely spreads, but it can damage nearby tissue if untreated.1
- It is highly curable. Surgery has the lowest recurrence rates; creams, freezing, light treatment, and radiation fit specific lower-risk situations.2
- A biopsy confirms the diagnosis, and because new spots and recurrences can appear years later, ongoing skin checks matter.3
What is basal cell carcinoma?
BCC is a cancer of the basal cells in the outer layer of skin. The main cause is years of ultraviolet light, from the sun or tanning beds. It is very common. One large study estimated more than 5 million non-melanoma skin cancers treated in the United States in a single year, and basal cell carcinoma is about half of those.1
How BCC behaves is what makes it both serious and very treatable. It grows slowly, and it rarely spreads to other organs. The harm comes from local growth. On the face, a tumor left alone can damage the skin, cartilage, and tissue near the eyes, nose, and ears. So it is treated even though it rarely spreads.4
Signs and what to look for
Basal cell carcinoma can look like several things, so any spot that is new, changing, or not healing is worth checking. Common signs include:
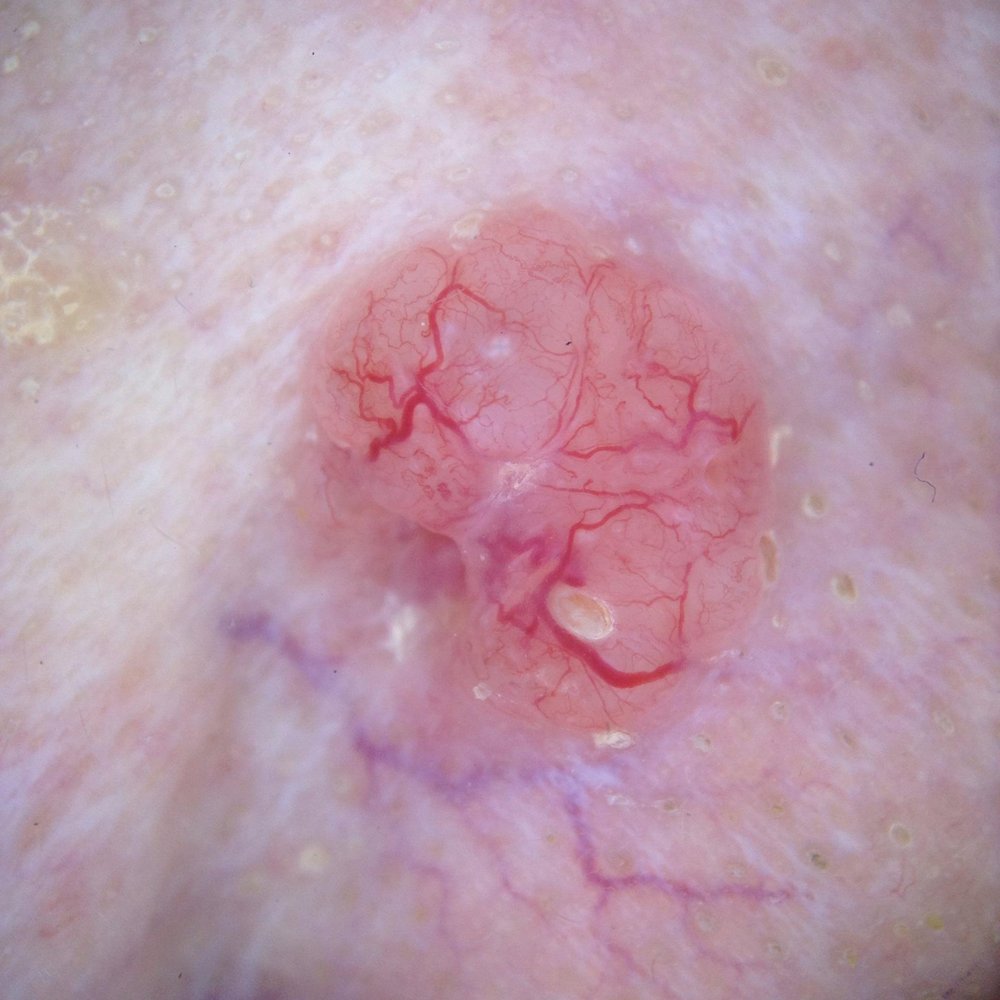
- A pearly or shiny bump, sometimes with tiny visible blood vessels
- A flat, scaly, reddish patch
- A sore that bleeds, scabs, heals, and comes back in the same place
- A waxy, scar-like area with poorly defined edges
These can appear skin-colored, pink, brown, or black. A spot that keeps bleeding or will not heal is a classic clue.
How it is diagnosed
Diagnosis starts with a skin exam, often using a handheld magnifier (dermoscopy). The diagnosis is confirmed with a biopsy, where a small sample is taken and checked under the microscope. The biopsy also tells the type, or subtype, of BCC, which guides treatment.3
Tumors are then sorted into lower-risk and higher-risk groups. That group drives the choice of treatment. A BCC is higher-risk if it has an aggressive type under the microscope, sits on the central face, is large, has fuzzy borders, has come back before, or grows in someone with a weak immune system.4
How it is treated
Most basal cell carcinomas are cured with treatment done in the office. The right option depends on the tumor's risk group, size, location, and your preferences. Here is how the options compare, strongest evidence first.
Surgery is the standard for most BCC. It has the lowest recurrence rates of any option.2 For high-risk, recurrent, or central-face tumors, a margin-controlled technique called Mohs surgery checks the whole edge of the removed tissue under the microscope during the visit. In a 10-year trial of high-risk facial BCC, recurrence after standard surgery was about 12% for new tumors and 14% for returning ones; with the margin-controlled technique it was about 4%. The difference was clear for returning tumors but not for new ones.56 Guidelines save the margin-controlled approach for those higher-risk cases.4
For small, low-risk surface tumors, other options can work when surgery is declined or not practical. These include a prescription cream (imiquimod), freezing or scraping-and-cautery, and light treatment (photodynamic therapy). They clear fewer tumors and come back more often than surgery, but can leave a better cosmetic result.7 Radiation is an option too, often for older patients or when surgery is not a good fit, though it comes back more than surgery.2
A small number of BCCs grow deep or spread and cannot be treated by surgery or radiation. These are treated with pills (hedgehog inhibitors) or, in some cases, immunotherapy. That care is given through a referral to a specialist who treats systemic cancer (a medical oncologist).8
Lowering your risk and catching new ones early
Most basal cell carcinoma is caused by ultraviolet light from the sun and tanning beds, so reducing UV exposure over a lifetime lowers the risk.49 For people who have already had two or more skin cancers, a daily vitamin (nicotinamide) modestly lowered the rate of new non-melanoma skin cancers in a trial.
Ultraviolet light from the sun and tanning beds is the main cause of basal cell carcinoma, so reducing lifetime UV exposure — shade, protective clothing, sunscreen, and avoiding tanning beds — lowers the risk. (Daily sunscreen on its own was not shown to reduce BCC in a randomized trial, likely because BCC is tied to intense, early-life sun; its proven trial benefit is for squamous cell cancer and precancers.)
About 23% fewer new non-melanoma skin cancers overall at one year in high-risk patients. For basal cell carcinoma on its own the evidence is mixed: the trial’s 20% drop was not statistically significant, and pooled analyses disagree, with one finding a significant reduction and another finding none. The benefit only lasts while you take it.
Whole-body prevention, separate from the spot treatments above. “No effect” means good trials found no benefit. Every source is PubMed-verified; not medical advice.
Having one basal cell carcinoma raises the chance of getting another, and some recurrences appear more than five years later, so regular skin checks are an important part of care after a diagnosis.5
When to see a doctor
See a clinician for any spot that is new, changing, bleeding, or not healing, especially a sore that heals and comes back in the same place. If you have already had a basal cell carcinoma, keep up with regular skin checks, since new spots and late recurrences can appear years later.
Worried about a spot?
SpotDoc offers full-body skin cancer screening in Brownwood Square, The Villages. No referral needed for most plans.
Frequently asked questions
Is basal cell carcinoma dangerous? It is rarely life-threatening because it almost never spreads to other organs. The concern is local growth: left untreated, it can damage nearby skin, cartilage, and tissue, especially on the face. Caught early, it is highly curable.4
Will it come back after treatment? Most tumors are cured, and surgery has the lowest recurrence rates.2 Some recurrences appear more than five years later, and having one BCC raises the chance of getting another, so ongoing skin checks matter.5
Can I treat it with a cream instead of surgery? For small, low-risk surface tumors, a prescription cream is an option, but it cures fewer tumors than surgery. In a head-to-head trial, 3-year success was 84% with imiquimod cream vs 98% with surgery.7 Creams are not used for higher-risk or deeper tumors.
What is Mohs surgery, and do I need it? It is a margin-controlled technique that checks the whole edge of the removed tissue under the microscope during the procedure. Guidelines reserve it for high-risk, recurrent, or critical-site tumors rather than every BCC.4 Your clinician can tell you whether your tumor falls into that group.
Does basal cell carcinoma spread? Very rarely. Spread to lymph nodes or other organs happens in a small fraction of cases. The usual concern is the tumor growing into nearby tissue, not spreading through the body.4
Questions to ask your clinician
- What risk group is my tumor, and how does that change my options?
- Which treatment fits this spot, and what will the scar or healed area look like?
- Will the removed tissue be checked for clear edges?
- How often should I have skin checks now that I have had a BCC?
- What can I do to lower my risk of new skin cancers?
Basal cell carcinoma is one of several skin cancers and precancers. Related guides cover squamous cell carcinoma, actinic keratosis, and the treatments above, including surgical excision. A thorough skin cancer screening is the place to start.
Reviewed by Tyler Long, DO. Last reviewed 2026-06-24.
Update log
How this guide has changed since it was first published.
- June 30, 2026Guide published.
References
Every statement on this page is backed by the peer-reviewed sources below — each links to the original study. Numbers match the citations in the text and the grids above.
- Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. population, 2012. JAMA Dermatol. 2015;151(10):1081–1086.View source
- Thomson J, Hogan S, Leonardi-Bee J, Williams HC, Bath-Hextall FJ. Interventions for basal cell carcinoma of the skin. Cochrane Database Syst Rev. 2020;11(11):CD003412.View source
- Kim JYS, Kozlow JH, Mittal B, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540–559.View source
- Peris K, Fargnoli MC, Garbe C, et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur J Cancer. 2019;118:10–34.View source
- van Loo E, Mosterd K, Krekels GAM, et al. Surgical excision versus Mohs’ micrographic surgery for basal cell carcinoma of the face: a randomised clinical trial with 10 year follow-up. Eur J Cancer. 2014;50(17):3011–3020.View source
- Mosterd K, Krekels GAM, Nieman FH, et al. Surgical excision versus Mohs’ micrographic surgery for primary and recurrent basal-cell carcinoma of the face: a prospective randomised controlled trial with 5-years’ follow-up. Lancet Oncol. 2008;9(12):1149–1156.View source
- Bath-Hextall F, Ozolins M, Armstrong SJ, et al. Surgical excision versus imiquimod 5% cream for nodular and superficial basal-cell carcinoma (SINS): a multicentre, non-inferiority, randomised controlled trial. Lancet Oncol. 2014;15(1):96–105.View source
- Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012;366(23):2171–2179.View source
- Leiter U, Garbe C. Epidemiology of melanoma and nonmelanoma skin cancer: the role of sunlight. Adv Exp Med Biol. 2008;624:89–103.View source
- Nagore E, Grau C, Molinero J, Fortea JM. Positive margins in basal cell carcinoma: relationship to clinical features and recurrence risk. A retrospective study of 248 patients. J Eur Acad Dermatol Venereol. 2003;17(2):167–170.View source
- Williams HC, Bath-Hextall F, Ozolins M, et al. Surgery versus 5% imiquimod for nodular and superficial basal cell carcinoma: 5-year results of the SINS randomized controlled trial. J Invest Dermatol. 2017;137(3):614–619.View source
- Basset-Séguin N, Ibbotson SH, Emtestam L, et al. Topical methyl aminolaevulinate photodynamic therapy versus cryotherapy for superficial basal cell carcinoma: a 5-year randomized trial. Eur J Dermatol. 2008;18(5):547–553.View source
- Dummer R, Guminski A, Gutzmer R, et al. Long-term efficacy and safety of sonidegib in patients with advanced basal cell carcinoma: 42-month analysis of the randomized phase 2 BOLT study. Br J Dermatol. 2020;182(6):1369–1378.View source
- Stratigos AJ, Sekulic A, Peris K, et al. Cemiplimab in locally advanced basal cell carcinoma after hedgehog inhibitor therapy: an open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2021;22(6):848–857.View source
- English DR, Armstrong BK, Kricker A, Fleming C. Sunlight and cancer. Cancer Causes Control. 1997;8(3):271–283.View source
- Chen AC, Martin AJ, Choy B, et al. A Phase 3 Randomized Trial of Nicotinamide for Skin-Cancer Chemoprevention. N Engl J Med. 2015;373(17):1618–1626.View source
- Mainville L, Smilga AS, Fortin PR. Effect of Nicotinamide in Skin Cancer and Actinic Keratoses Chemoprophylaxis, and Adverse Effects Related to Nicotinamide: A Systematic Review and Meta-Analysis. J Cutan Med Surg. 2022;26(3):297–308.View source
- Tosti G, Pepe F, Gnagnarella P, et al. The Role of Nicotinamide as Chemo-Preventive Agent in NMSCs: A Systematic Review and Meta-Analysis. Nutrients. 2023;16(1):100.View source